80 year old man with C/O fever and pedal edema.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
80 year old man from Dattaiahgudem, Mothkur mandal presented to casuality with chief complaints of pedal edema from 10 days. Complaint of fever 15 days back intermittent type not associated with cough, cold, vomitings. Fever subsided five days back after which patient developed reduction in urine output. Patient also complained of grade 2 to grade 3 dyspnea along with pedal edema. Patient was apparently asymptomatic 15 days back when he developed intermittent type of fever. Patients later on developed pedal edema involving both lower Limb gradually progressing upto knees. Patient also complained of itching over arms. Patient now complaints of reduced urine output from 4 days. Is not a known case of diabetes mellitus. Known case of hypertension since 1 year.
O/E :
Pallor +
Pedal edema pitting type present extending upto below knee.
No icterus, clubbing, lymphadenopathy .
BP :
PR : 92 bpm
RR : 20 cpm
CVS : S1, S2 heard, no murmurs
RS: Decreased breath sounds in Right and Left Supra clavicular areas.
Crepitations + B/L infrascapular areas.
P/A : soft, non tender, Bowel sounds heard.
CNS : Intact



2D echo reporting:
No RWMA
Moderate TR with PAH , Mild MR , Moderate AR
Sclerotic AV, No MS , Mild AS
EF = 54%
Fair LV systolic function
Diastolic dysfunction, no PE
IVC dilated ( 1.7 cms)
Dilated RA / LA
Mild dilated RV
Day 1:
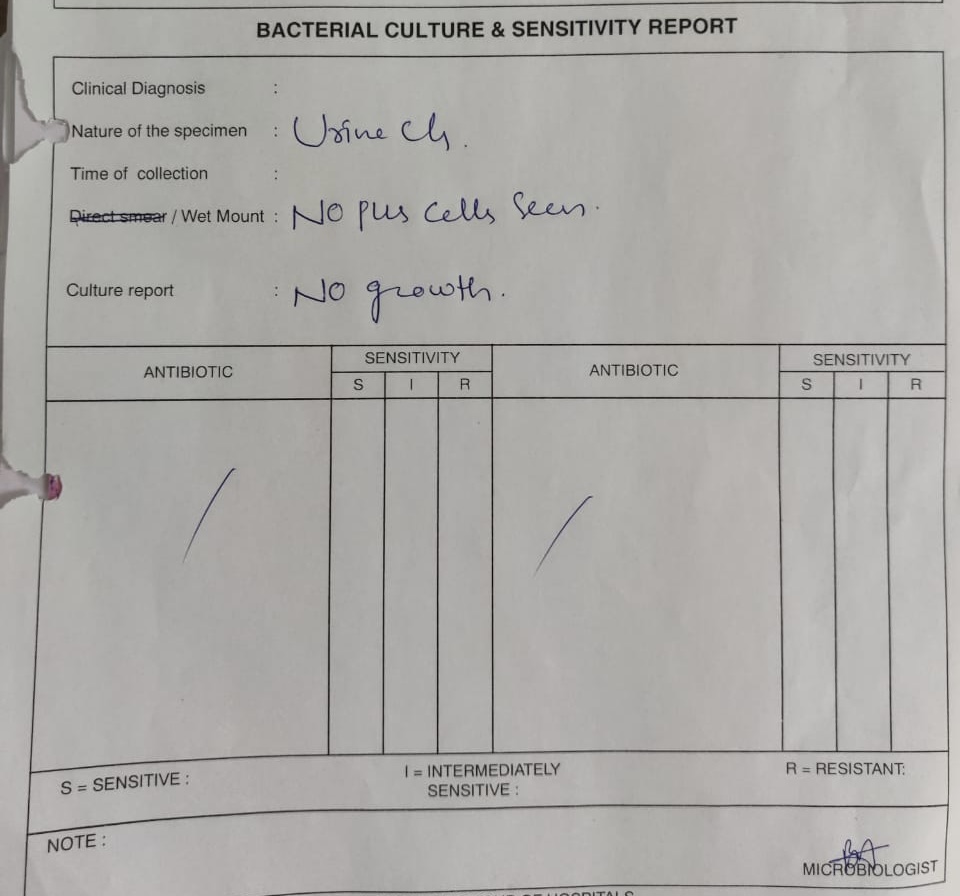
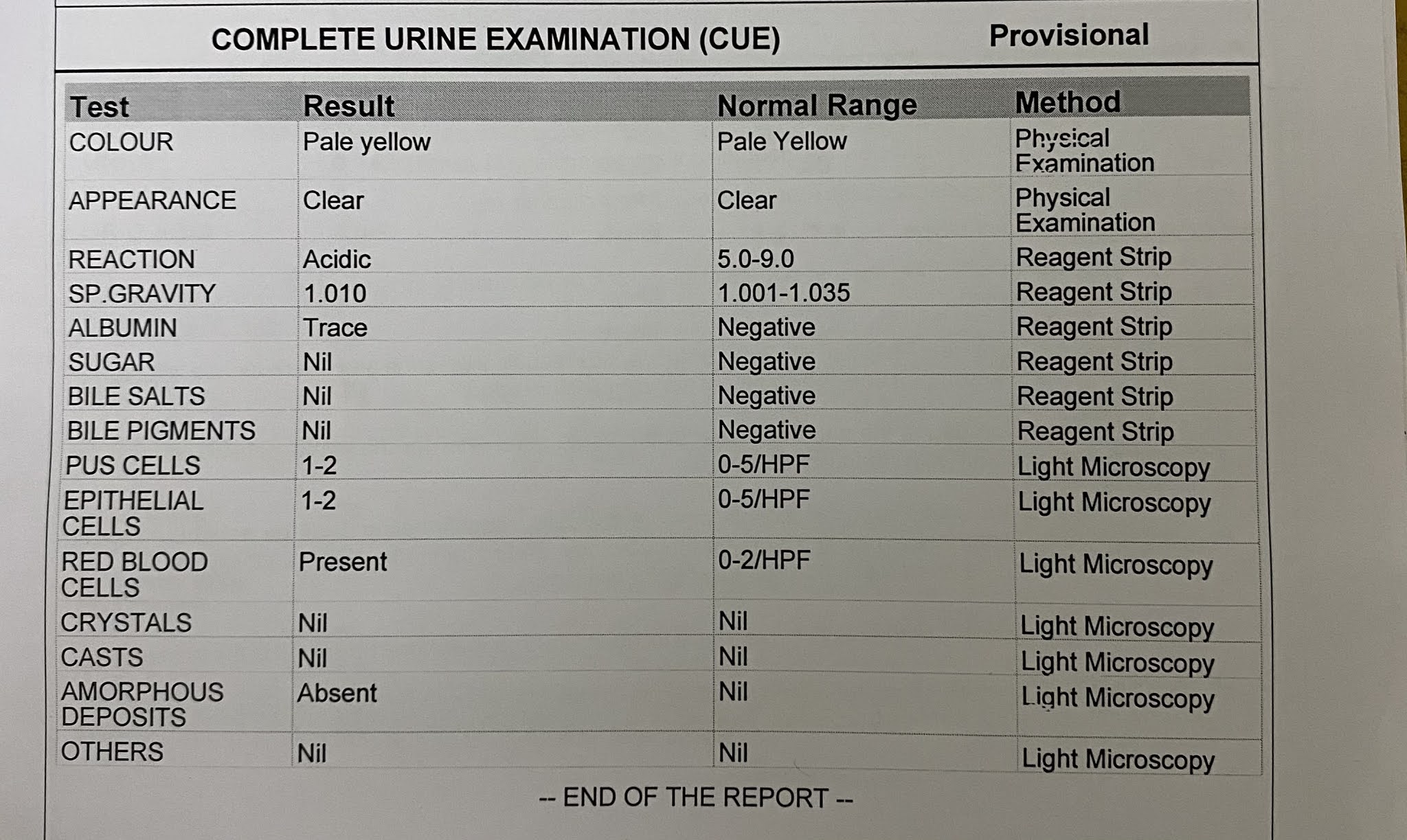
Investigations:






Inj Piptaz 4.5 gm IV / stat
Inj Piptaz 2.25 gm IV / TID
Inj Pan 40 mg IV / TID
Inj Lasix 40 mg IV / BD
IVF ——- NS @ UO + 30 ml/ hr
——— DNS
Tab Amlong 5 mg PO / OD
Tab PCM 650 mg PO / SOS
Day 2:


Inj Piptaz 2.25 gm IV / TID
Inj Pan 40 mg IV / TID
Inj Lasix 40 mg IV / BD
IVF ——- NS @ UO + 30 ml/ hr
——— DNS
Tab Amlong 5 mg PO / OD
Tab PCM 650 mg PO / SOS
Day 3 :


Inj Piptaz 2.25 gm IV / TID
Inj Pan 40 mg IV / TID
Inj Lasix 40 mg IV / BD
Tab Amlong 5 mg PO / OD
Tab PCM 650 mg PO / SOS
Inj Optineuron 1 Amp in 100 ml NS / IV / OD
Day 4:







Inj Piptaz 2.25 gm IV / TID
Inj Pan 40 mg IV / TID
Inj Lasix 40 mg IV / BD
Tab Amlong 5 mg PO / OD
Tab PCM 650 mg PO / SOS
Inj Optineuron 1 Amp in 100 ml NS / IV / OD
Syp Citralka 10 ml in 1 glass of water / TID
Tab Levocitrizine 10 mg PO / HS
Day 5 :
Inj Piptaz 2.25 gm IV / TID
Inj Pan 40 mg IV / TID
Inj Lasix 40 mg IV / BD
Tab PCM 650 mg PO / SOS
Inj Optineuron 1 Amp in 100 ml NS IV / OD
Tab Cilindipine 5 mg PO / OD at 8 AM
Syp Citralka 10 ml in 1 glass of water / TID
Syp Cremaffin 10 ml PO / BD
Tab Levocitrizine 10 mg PO/ HS
Patient was discharged on Day 6.
He was subjectively feeling better.
His pedal edema reduced compared to the day of presentation.
He was advised to continue these medications:
Tab Lasix PO/ TID X 1 week
Tab Cilindipine 5mg PO/ OD at 8 AM. X 1 week
Syp Citralka 10 ml in 1 glass of water / TID X 1 week
Syp Cremaffin sulfate 10 ml PO/ BD X 1 week
Tab Levocitrizine 10 mg PO / HS X 5 days
Tab Orofer XT PO / OD X 1 week
Tab Neurobion forte PO/ OD X 1 week
Patient was advised to review after 1 week.


Comments
Post a Comment