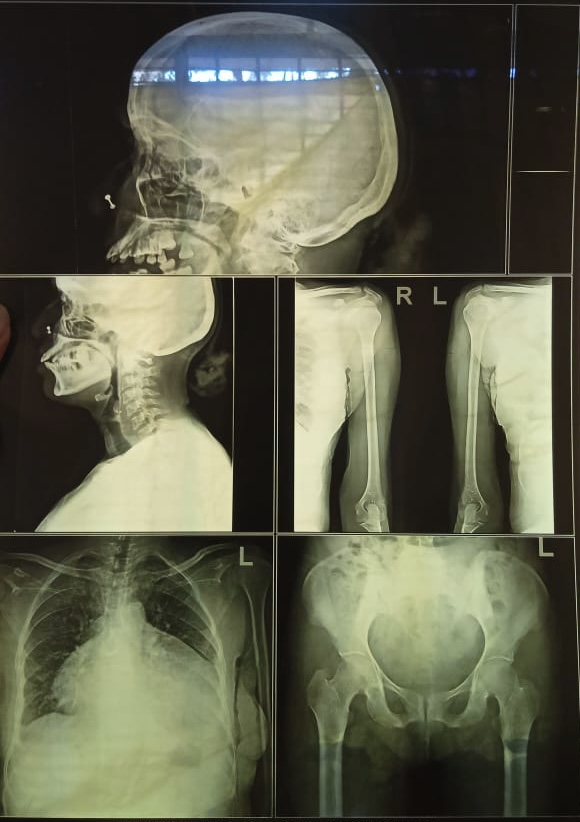
56/F with C/O Chest pain, generalised weakness.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
56 year old female from Ammanabolu, Tobacco leaf seller by occupation came with chief complaints of Decreased appetite since 20 days, generalised weakness since 15 days , Pain abdomen since 10 days. B/L Lower limb ,upper limb edema and facial puffiness since 5 days. She recalled having on and off chest pain since 6 months, pricking type, subsiding on its own, no radiation.
Palpitations + Syncopal attacks -
15 days back patient had loose stools 10-15 episodes per day small in quantity associated with pus, foul smelling, not associated with blood and associated with pain abdomen and fever and nausea and loss of taste and these lasted for 2 days and relieved after using some medication given by local RMP. After using medication for 3 days she experianced same complaints of diarrhoea which lasted for 2 days 15 episodes per day.
Since then she developed generalised weakness, malaise, fatigue.
SOB since 1 month, gradual in onset, gradually progressed to Grade IV, aggravated on exertion, relieved on rest initially ( not relieving now). No orthopnoea or PND.
Patient also complaining of head ache since 10 days, B/L frontal region, photophobia - , phonophobia -
Giddiness +
Pain abdomen since 10 days - squeezing type, relieved on taking food, non radiating .
She is not a K/C/O DM - II , HTN.
She is an occasional alcoholic ( beer / whiskey) since 35 years. Chews tobacco leaves daily since 6 months.
O/E:
Patient is C/C
Pallor +
No icterus, clubbing , cyanosis, lymphadenopathy
No significant pedal edema.
Temp - 98.6 F
PR - 108 bpm
BP - 120/70 mm of Hg
Spo2 - 98 %
CVS - Parasternal heave +
S1 , S2 +
Loud P2 in Pulmonary area.
Pansystolic murmur in Tricuspid area.
Pulsus parodoxus + (12 mm Hg)
Bamberger sign +
Rotch sign +
Raised JVP prominent X descent - 14 cms.
RS - BAE + , fine inspiratiry crepts present in right and left ISA
P/A - distended , multiple hemorrhagic spots seen. Hepatomegaly present with liver span of 15 cm
Tenderness + in epigastric and Right hypochondric area.


Out side report as of 14-1-2021 :
Hb - 4.2 gm/dl
Wbc - 7500
Platelet - 1.06 lakhs
Out side 2D echo:
Moderate TR
Severe PAH
Moderate Pericardial effusion.
Diagnosis: Severe Anaemia under evaluation with moderate Pericardial effusion with PAH
Day 1 :

2D echo showed pericardial effusion with Diastolic RV collapse.
Pericardial tap was done and 100 ml was aspirated.
Post Pericardiocentesis
2D echo :
ECG:

After 20 min patient developed Hypotension. BP - 60/40 mm Hg
PR - 102 bpm
Patient was given
1)IVF NS bolus
2) Inj NorAdrenaline 2amp in 45 ml NS @ 6ml per hour
⬇️
BP - 100 /70 mm Hg
1) IVF NS/ RL @ 75 ml/hr
2) Inj NorAdrenaline @ 6ml/hr
⬇️
BP - 110/70 mm Hg
ECG :











































Comments
Post a Comment