67 Year old female with C/o involuntary movements of both upper limbs.
This is an online E log book to discuss our patient's
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
67 year old woman presented with the complaints of
Involuntary movements of right forearm since 4 months.
Involuntarily movements of left index finger and thumb since 4 months.
Patient lives at Haliya in Nalgonda district and is married to a coolie. She has 3 daughters and 4 sons.
She had a hysterectomy 30 years back.
She got diagnosed to be hypertensive and diabetic 3 years ago but hasn’t been regularly taking her medications.
Since 4 months , her husband started noticing involuntary movements of her right forearm which would be more at rest and would also be present during her sleep. Over the next few days, she developed involuntary movements of her left Index finger and thumb following which she even developed on and off involuntary movements of her tongue.
Since the last 20 days, he says she hasn't been involving herself in conversations and would respond late.
On examination:
PR - 76bm
Bp - 120/80mmhg in supine posture
110/70mmg on standing
Clinical Findings:
Masked like facies.
Asymmetrical rhythmic movements of distal muscles - right forearm and pill rolling tremors observed involving left thumb and index finger, occuring even at sleep.
Small amplitude.
Tremors present on rest and absent on motor activity.
Slow initiation of motor activity and delayed verbal response.
Lead pipe rigidity present.
Power - 4- in all the four limbs
Reflexes. Rt Lt
B. 3+. 3+
T. 3+. 3+
S. 3+. 3+
K. 3+. 3+
A. - -
P Flexion.
Gait: Short steps, Reduced arm swing.
HINTS: No delayed saccades on Head Impulse,
No nystagmus noted,
Test for Vertical skew - Negative
MMSE:
Orientation : 5/5
Registration: 3/5
Attention and Calculation : Doesn’t know how to calculate.
Recall : 3/5
Language: Name two objects- 2/2
No ifs and buts - 1/1
Three stage command - 3/3
Read a written command - unable to ellicit.
Write a sentence- unable to ellicit.
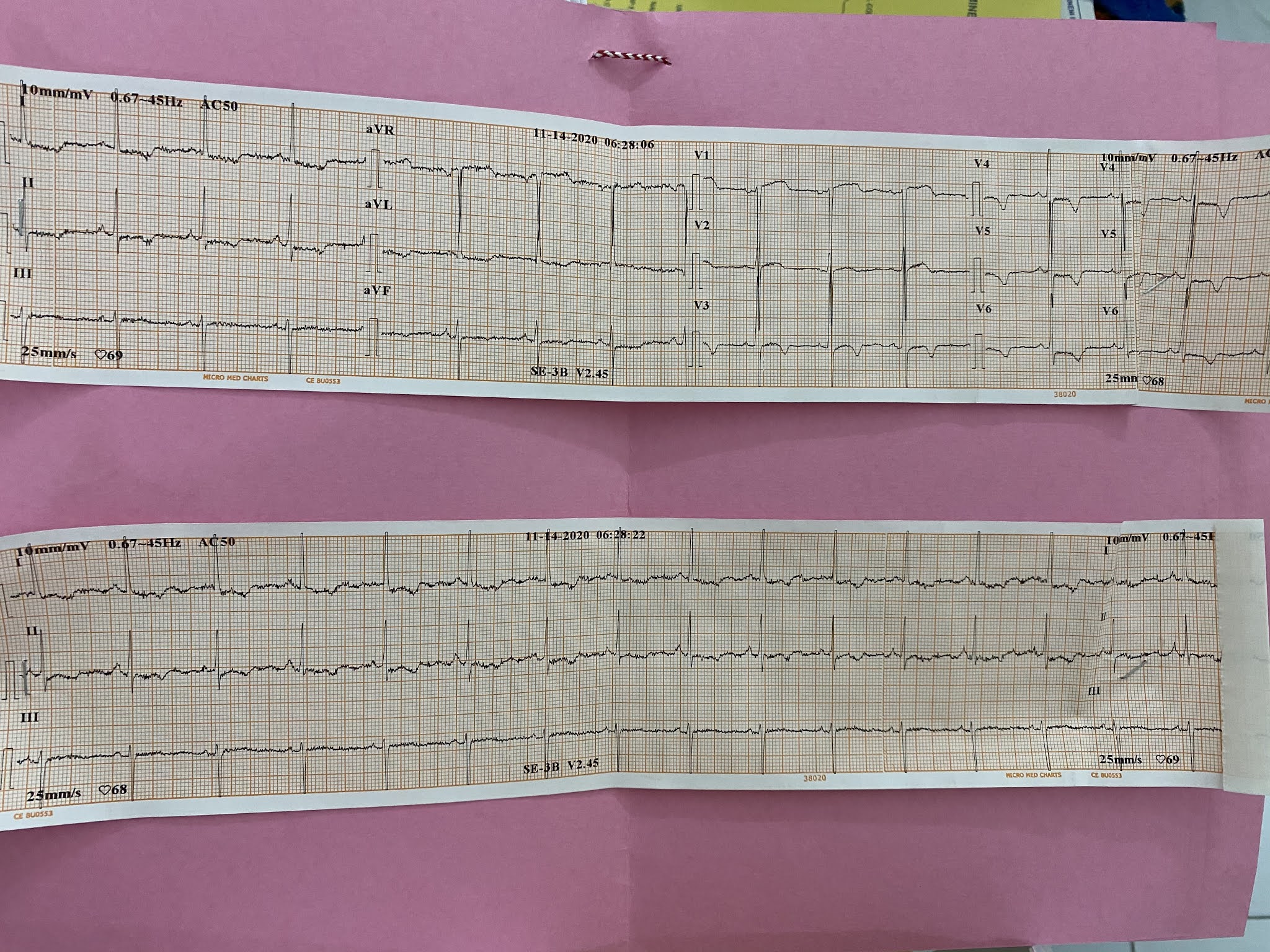
CVS:
Loud ejection systolic murmur heard in aortic area till apex.
The following video shows pill rolling tremor.
In the following video we can see the reduced arm swing.



















Carbidopa is a drug that blocks conversion of levodopa to dopamine outside of central nervous system (CNS) and thus inhibits unwanted side effects of levodopa on organs located outside of CNS during management of Parkinson's Disease (PD). PD is associated with increased expression of inflammatory genes in peripheral and central nervous system (CNS), infiltration of immune cells into brain, and increased numbers of activated/memory T cells. Animal models of PD have shown a critical role of T cells in inducing pathology in CNS. However, the effect of carbidopa on T cell responses in vivo is unknown.
In this report, we show that carbidopa strongly inhibited T cell activation in vitro and in vivo. Accordingly, carbidopa mitigated myelin oligodendrocyte glycoprotein peptide fragment 35-55 induced experimental autoimmune encephalitis and collagen induced arthritis in animal models. The data presented here suggest that in addition to blocking peripheral conversion of levodopa, carbidopa may inhibit T cell responses in PD individuals and implicate a potential therapeutic use of carbidopa in suppression of T cell mediated pathologies.


Comments
Post a Comment